Enlace a entrada en español
Extracts of the Presentation to the International Society for Geographic and Epidemiologic Ophthalmology by David Dunaway and Ian Berger (InFOCUS Center for Primary Eye Care Development).
[…] Estimates of the number of people worldwide with refractive error range from about 800 million to 2.3 billion. No prevalence data are available from the World Health Organization or from any other source relating to very large populations such as groups of nations, or whole countries. […]
[…] As for the proportion of an entire population with refractive error, Daniel Etyale of the W.H.O. reported at a special session on refractive error at an International Agency for Prevention of Blindness meeting in 2001, that 5 -15 percent of children are considered to have refractive errors, the majority of which are uncorrected, and that there is currently a need for population based studies to ascertain these figures. […]
[…] Although sufficient data have not been collected to accurately predict prevalence per diopter of correction for most populations, general prevalence information on the three types of refractive errors and of presbyopia can provide an orientation of what to expect.
- Hyperopia, for example, is usually present at birth, except in premature infants. Hyperopia decreases in magnitude through age 4 years, and the prevalence of hyperopia less than +1.25 D (an amount usually difficult to compensate accomodatively) is 4-7 percent between ages 5-20 years, remains constant through early middle age, then increases in populations aged 45 or more. […] Hyperopia also occurs in patients with poorly controlled diabetes and in patients who've had cataract surgery.
- Myopia prevalence varies with age, race and sex, increasing at least through adolescence, and is present in 1 per cent of children at age 5 years, increasing to 8 per cent at age 10 years and about 15 per cent at 15 years. Myopia occurs slightly more frequently in females than in males.
- The prevalence of astigmatism may be as high as 70 per cent, if all amounts are included, but is considered to decrease to 3 percent if the extent is limited to 1.25 diopters or more. […] If astigmatism is greater than 1 diopter, it usually develops before age 2 years.
- Not a refractive error, presbyopia is due to a loss of accommodative ability. It usually starts between ages 38-45 years and the prevalence is 100 percent by age 55. Early onset is associated with hyperopia. […]
RELATED POSTS
Refractive visual disorders. Some clarifications.
Monday, December 29, 2008
Thursday, December 11, 2008
Refractive visual Disorders. Some clarifications.
Enlace a entrada en español
As I wrote in the previous post, when we assess somebody’s Visual Acuity and the result obtained is not 20/20, it may be, among other reasons, because of the presence of some “ametropia” also called “refractive eye disorder” or “refractive error”.
But before explaining what these words mean, first I will explain what Ocular Refraction is: it is a physical phenomenon where the light rays from the object that we look at and from the whole visual field surrounds it, when crossing certain optical structures of the eye, change their path to focus on the fovea (13) and certain points of the retina. There, these light stimuli are converted into nervous stimuli which are sent to the brain (occipital lobe) in order to convert the information from the both eyes into simple and clear image of the target and all that surrounds it.
As I wrote in the previous post, when we assess somebody’s Visual Acuity and the result obtained is not 20/20, it may be, among other reasons, because of the presence of some “ametropia” also called “refractive eye disorder” or “refractive error”.
But before explaining what these words mean, first I will explain what Ocular Refraction is: it is a physical phenomenon where the light rays from the object that we look at and from the whole visual field surrounds it, when crossing certain optical structures of the eye, change their path to focus on the fovea (13) and certain points of the retina. There, these light stimuli are converted into nervous stimuli which are sent to the brain (occipital lobe) in order to convert the information from the both eyes into simple and clear image of the target and all that surrounds it.
 This change of the light path is mainly due to two structures which act as lens into the eye: the cornea (1) and the crystalline lens (8) . And to a lesser extent: the aqueous humor (4) (in the anterior and posterior chamber) and the vitreous body (9) (inside of the vitreous chamber), which also influence the “dioptric power” of the eye.
This change of the light path is mainly due to two structures which act as lens into the eye: the cornea (1) and the crystalline lens (8) . And to a lesser extent: the aqueous humor (4) (in the anterior and posterior chamber) and the vitreous body (9) (inside of the vitreous chamber), which also influence the “dioptric power” of the eye. Therefore, when the image of an object, placed at 20 feet (6 meters), is focused on the retina of an eye, it shows that this eye is emmetrope and its Visual Acuity (if it does not have any pathologic disorder that hampers it) will be 20/20 or better. That is, this eye does not suffer any refractive eye disorder.
Therefore, when the image of an object, placed at 20 feet (6 meters), is focused on the retina of an eye, it shows that this eye is emmetrope and its Visual Acuity (if it does not have any pathologic disorder that hampers it) will be 20/20 or better. That is, this eye does not suffer any refractive eye disorder.
But if the two following conditions are fulfilled:
- its Visual Acuity is lower than 20/20
- and it improves with the help of eyeglasses, contact lenses or another optical option,
then we can catalog this eye disorder as “Refractive Error” or “Ametropia”. This disorder is due to an upset in the power of either one of or both lenses (surfaces more curved in the case of the myopia and more flat in the case of the hypermetropia), or a change of the eye axial length (the eye is too short in the case of the myopia and too long in the case of the hypermetropia): Grosso modo, I will now explain the refractive eye disorders, but in later posts I will explain each one of them in detail.
Grosso modo, I will now explain the refractive eye disorders, but in later posts I will explain each one of them in detail.
MYOPIA: It is the refractive error that is better known, worldwide. This prevents the distant objects to be clearly seen. In this case, optically, the light rays from the distant object (placed at 20 feet -6 meters-), are focused in a point in front of the retina, so the image is blurred.
HYPERMETROPIA or HYPEROPIA: This refractive error prevents the nearby objects, and sometimes the distant ones too, to be clearly seen. In this case, optically, the light rays from this object are focused in a point behind of the retina; so, as with the myopic eye, the hypermetropic one also sees the image blurred.
But the difference with the myopic eye is that this defect of vision is more unnoticed, and it is a defect no so well-known by people, because of the modifications that the crystalline lens can perform of its curvature, so this lens can compensate part or all of this hypermetropia ( if this is not very high) so it remains latent.
It is the most common refractive error in the newborn, because when the baby is born, the eye is not completely developed and as the body grows, so does the eyes. So, a baby with a small hypermetropia may turn into an emmetrope when she grows.
ASTIGMATISM: In the previous refractive errors, the cornea is a spherical structure (as if it was an inflated basketball that we have cut in half). However, in this defect of vision the cornea can be seen as an American football also cut in half. Therefore, each curve in the cornea has a different dioptric power (I will better explain this concept later) and consequently, the light rays that cross each curvature suffer a different change of direction, and causing a focusing of the image on different points regarding to the retina, causing not only a blurred image but also a drop-shadow effect in the surroundings of the distant and/or nearby images. Because of this reason, the astigmatism can co-exist with myopia or hypermetropia in the same eye, but these last errors can not co-exist in the same eye at the same time.
Therefore, each curve in the cornea has a different dioptric power (I will better explain this concept later) and consequently, the light rays that cross each curvature suffer a different change of direction, and causing a focusing of the image on different points regarding to the retina, causing not only a blurred image but also a drop-shadow effect in the surroundings of the distant and/or nearby images. Because of this reason, the astigmatism can co-exist with myopia or hypermetropia in the same eye, but these last errors can not co-exist in the same eye at the same time.
All these refractive eye disorders cause a “faulty vision”, but in these cases this is only due to a wrong Visual Acuity. That’s why, VISION and VISUAL ACUITY are not the same concept, because we can have a value 20/20 of Visual Acuity and not being able to read the registration number of the car in front of us at 2 meters (6 feet) or keep on reading for 1 hour. Visual Acuity is only one of the different features of vision.
These “ametropias” are primary; secondarily, other refractive eye disorders may also arise:
ANISOMETROPIA: It is very strange to find a person with the same quantity of ametropia in both eyes (because we do not have two identical eyes), but anisometropia is the condition in which this difference is so big, that it is difficult that the information from the images from each eye that arrive to the brain, can be fused (I will explain this better) and can create a simple clear image.
AMBLYOPIA: It more well-known as “LAZY EYE”. This may be related to the previous disorder. I am sure some time you had seen a child wearing a patch at school or in the street, since this is one of the many ways to treat this problem (I will explain this one too).
In this case, the difference of eyeglass prescription and the functional features of one eye may be very different from the other, so one of them develops better. In this case the early diagnosis and treatment is VERY IMPORTANT.
PRESBYOPIA: Sooner or later everybody will “suffer” from this ametropia, even the person that think that, while being young, has got the best vision of the world… Sorry
This is just because of the natural aging process of human body. As time goes by we keep on losing our forces and things we could perform some years ago, now we are not capable of doing them; in vision the same fact happens too. Inside the eye, the muscle that controls the change of focus for different distances, by modifying the curvature of crystalline lens, “is more tired” too and keeps on losing flexibility, force and speed of response. As time goes by we have more difficulty for focusing more quickly and we can not see small details of nearby objects. The arms seem to stretch more and more and we would wish we’d have them longer in order to read a medicine directions for use or just a newspaper. In this case, the problem we have I resides in nearby tasks.
In the other hand, there are other disorders that also cause reduced Visual Acuity, but the difference is that this value can not be improved with any optical option, they are not refractive eye disorders but pathological disorders: Cataract, Macular Degeneration, Glaucoma ... In these cases the required treatment can not be offered by the optometrist (medicines and surgeries).
Besides there are defects of vision that are independent of the Visual Acuity value, such as, for instance: a reduced visual field, a disorder of color vision, a problem in order to focus in an efficient way when we read a book, or to work with both eyes as a team, or to discriminate shapes, or to remember what we see, or to copy something we see, or to follow a straight line… Therefore, these are not disorders of the Visual Acuity.
ILYD
RELATED POSTS
Refractive disorders: Hyperopia , Hypermetropia or Farsightedness. (1) Vision and Accommodation
MyopiaRefractive disorders: Myopia or Nearsightedness (1) Vision and Symptoms
Some numbers...
Wednesday, October 29, 2008
A good vision is not only seeing 20/20
Enlace a entrada en español
 Just as “seeing” is not the same as “looking”, talking about vision it is not only enough that light focuses in a specific point of the retina in order to see 20/20, but also, vision is understanding what we see.
Just as “seeing” is not the same as “looking”, talking about vision it is not only enough that light focuses in a specific point of the retina in order to see 20/20, but also, vision is understanding what we see.
In order to understand this concept, I will firstly explain what the words Visual Acuity mean, that many times we utilize them with our patients when we say “You have 20/20 vision“, but maybe you are not quite sure what actually that means.
When we assess the Visual Acuity test, we are assessing the ability that someone has to identify some letters or patterns from a distance where they should be seen; and the final value is the smallest symbol size than the patient is able to read from that distance.
 Let me explain it better: when we perform this test, the patient must sit down 20 feet (6 meters) away from the letters chart. When we say that a person have 20/20 visual acuity (100%, 1.0 or 6/6, everything is the same), what we mean is that the person sees 20 feet away from the chart what she should actually see 20 feet away. But for instance, if that person has 20/10 visual acuity (6/3 or 0.5), that means she would only see from 20 feet what she should see from 10 feet, that is, she has 50% of vision.
Let me explain it better: when we perform this test, the patient must sit down 20 feet (6 meters) away from the letters chart. When we say that a person have 20/20 visual acuity (100%, 1.0 or 6/6, everything is the same), what we mean is that the person sees 20 feet away from the chart what she should actually see 20 feet away. But for instance, if that person has 20/10 visual acuity (6/3 or 0.5), that means she would only see from 20 feet what she should see from 10 feet, that is, she has 50% of vision.

Therefore, Visual Acuity is the ability to see the details of an object. But precisely because that object is not floating in the void, but furthermore, there are many more objects surrounding it, we are in a distance from that object, we may want to execute an action with it and other senses may be implicated in this action…, vision is just not only clearly seeing that object, but that many more “visual qualities” might be implicated, as we saw in a previous post .
“It is estimated that as much as 80 percent of all learning during a child’s first 12 years comes through vision”.
Because a child or an adult has 20/20 visual acuity according to a certain test, it does not mean she has good vision, since she may have problems in order to focus on a text when she reads a book, or may have bad eye-hand coordination and consequently have a bad writing, or may have some problems to how her eyes work as a team and they feel tired 10 minutes after they start a near task, or may be "clumsy" and hit herself with things because she does not calculate the distances well. In all of these examples, vision is involved and with them I only wanted to show that although we have a 20/20 Visual Acuity maybe we do not have a 100% Vision.
In many optician’s, when a person goes to check her vision, they only obtain this result and only find out the lens required to improve that percentage (whether there is myopia, hypermetropia or astigmatism), without assessing if that vision works well and if it works along with the other senses. That is, for them the goal is to obtain 20/20 visual acuity and they do not think in any other symptom that shows that it is not only important to improve Visual Acuity, but also to improve the performance working at near, or practicing a sport or reading and its comprehension. For it, as the daily problems are not always related to a visual problem, I recommend you to go to a specialized office that offers you a broader eye examination. You would be surprised of how many symptoms and problems at school can be removed by using Visual Therapy, and what this can be done to improve the quality of life in general of any person.
A child may be diagnosed with a “perfect vision” by an optician or an ophthalmologist (it doesn’t matter) simply because she has 20/20 visual acuity, but without being assessed the necessary visual skills (focusing, peripheral vision, eye-hand coordination, discrimination of shapes, spatial relations,…) required to have a correct learning or a good physical coordination. In a later post I will thoroughly explain the visual problems related with learning.
If a child is struggling with academics, sports or home behavior, parents and teachers should be encouraged to consider that a vision problem may exist, beyond a Visual Acuity.
 A simple comparative example is the following one: when we read, it is not enough to verbalize what we see written and to read as a parrot, we have to understand what we see. Therefore, when we read, we must not only clearly see the letters, but we have to know, to remember, to interpret and verbalize what is written; vision process is responsible for all this.
A simple comparative example is the following one: when we read, it is not enough to verbalize what we see written and to read as a parrot, we have to understand what we see. Therefore, when we read, we must not only clearly see the letters, but we have to know, to remember, to interpret and verbalize what is written; vision process is responsible for all this.
So, after all this, mi goal is for you to have a clear understanding that when you go to an office or optician’s, the Visual Acuity assessment must be ONLY a value obtained of the whole visual examination in order to achieve a precise diagnosis.
BOOK: "20/20 is not enough"
 Just as “seeing” is not the same as “looking”, talking about vision it is not only enough that light focuses in a specific point of the retina in order to see 20/20, but also, vision is understanding what we see.
Just as “seeing” is not the same as “looking”, talking about vision it is not only enough that light focuses in a specific point of the retina in order to see 20/20, but also, vision is understanding what we see.In order to understand this concept, I will firstly explain what the words Visual Acuity mean, that many times we utilize them with our patients when we say “You have 20/20 vision“, but maybe you are not quite sure what actually that means.
When we assess the Visual Acuity test, we are assessing the ability that someone has to identify some letters or patterns from a distance where they should be seen; and the final value is the smallest symbol size than the patient is able to read from that distance.
 Let me explain it better: when we perform this test, the patient must sit down 20 feet (6 meters) away from the letters chart. When we say that a person have 20/20 visual acuity (100%, 1.0 or 6/6, everything is the same), what we mean is that the person sees 20 feet away from the chart what she should actually see 20 feet away. But for instance, if that person has 20/10 visual acuity (6/3 or 0.5), that means she would only see from 20 feet what she should see from 10 feet, that is, she has 50% of vision.
Let me explain it better: when we perform this test, the patient must sit down 20 feet (6 meters) away from the letters chart. When we say that a person have 20/20 visual acuity (100%, 1.0 or 6/6, everything is the same), what we mean is that the person sees 20 feet away from the chart what she should actually see 20 feet away. But for instance, if that person has 20/10 visual acuity (6/3 or 0.5), that means she would only see from 20 feet what she should see from 10 feet, that is, she has 50% of vision.
Therefore, Visual Acuity is the ability to see the details of an object. But precisely because that object is not floating in the void, but furthermore, there are many more objects surrounding it, we are in a distance from that object, we may want to execute an action with it and other senses may be implicated in this action…, vision is just not only clearly seeing that object, but that many more “visual qualities” might be implicated, as we saw in a previous post .
“It is estimated that as much as 80 percent of all learning during a child’s first 12 years comes through vision”.
Because a child or an adult has 20/20 visual acuity according to a certain test, it does not mean she has good vision, since she may have problems in order to focus on a text when she reads a book, or may have bad eye-hand coordination and consequently have a bad writing, or may have some problems to how her eyes work as a team and they feel tired 10 minutes after they start a near task, or may be "clumsy" and hit herself with things because she does not calculate the distances well. In all of these examples, vision is involved and with them I only wanted to show that although we have a 20/20 Visual Acuity maybe we do not have a 100% Vision.
In many optician’s, when a person goes to check her vision, they only obtain this result and only find out the lens required to improve that percentage (whether there is myopia, hypermetropia or astigmatism), without assessing if that vision works well and if it works along with the other senses. That is, for them the goal is to obtain 20/20 visual acuity and they do not think in any other symptom that shows that it is not only important to improve Visual Acuity, but also to improve the performance working at near, or practicing a sport or reading and its comprehension. For it, as the daily problems are not always related to a visual problem, I recommend you to go to a specialized office that offers you a broader eye examination. You would be surprised of how many symptoms and problems at school can be removed by using Visual Therapy, and what this can be done to improve the quality of life in general of any person.
A child may be diagnosed with a “perfect vision” by an optician or an ophthalmologist (it doesn’t matter) simply because she has 20/20 visual acuity, but without being assessed the necessary visual skills (focusing, peripheral vision, eye-hand coordination, discrimination of shapes, spatial relations,…) required to have a correct learning or a good physical coordination. In a later post I will thoroughly explain the visual problems related with learning.
If a child is struggling with academics, sports or home behavior, parents and teachers should be encouraged to consider that a vision problem may exist, beyond a Visual Acuity.
 A simple comparative example is the following one: when we read, it is not enough to verbalize what we see written and to read as a parrot, we have to understand what we see. Therefore, when we read, we must not only clearly see the letters, but we have to know, to remember, to interpret and verbalize what is written; vision process is responsible for all this.
A simple comparative example is the following one: when we read, it is not enough to verbalize what we see written and to read as a parrot, we have to understand what we see. Therefore, when we read, we must not only clearly see the letters, but we have to know, to remember, to interpret and verbalize what is written; vision process is responsible for all this.So, after all this, mi goal is for you to have a clear understanding that when you go to an office or optician’s, the Visual Acuity assessment must be ONLY a value obtained of the whole visual examination in order to achieve a precise diagnosis.
BOOK: "20/20 is not enough"
Monday, October 06, 2008
An apple a day really does keep the doctor away
Enlace a entrada en español

This idiom is very famous, but we do not always heed this advice.
Prevention and Early Detection
Optometry basically detects visual upsets, that is, visual problems, performance problems related to vision, development problems related to vision, and so on. Therefore, if this detection is made as soon as possible, the treatment will be more effective, will need to carry out it less time and the results will be more lasting.
How can you know if you suffer any visual upset?
FROM THE FACT THAT THERE IS NO OCULAR PATHOLOGY OR ILLNESS, if you notice that you have some troubles in order to see at distance or at near (in order to read, write, draw, watch TV, drive, practice any sport, use a computer,…), this indicates that probably, you are suffering from some “refractive error” (myopia, hypermetropia, astigmatism, anisometropia, presbyopia... concepts that I will explain in later posts). These visual problems are not pathologies or eye illness, but they may cause a big discomfort performing the tasks of daily life, although they have an insignificant value.
These problems are “quantitative visual disorders”, and using a prescription (eyeglasses, contact lenses or prisms), usually they are corrected (THOUGH NOT REMOVED).
But, in the other hand, there are other “problems of quality vision” (they are not eye illness neither), that we can not be shown to the patient with understandable quantitative data, but that, however, may almost cause more frustration and powerlessness than the previous problems. This is because many people do not know very well what happened, or where they can go with their problem.
Fortunately, there are more and more optician’s shops or offices where they perform visual exams are more complete than a simple ocular refraction in order to obtain those “refractive errors”. There they detect the reason of it: a performance problem at work or at school, a learning disability, a visual development problem, a clumsiness or balance problem, an inability in order to read a book during long time, a carsick, a dyslexia, and so on. I guess that you did not imagine the great relation that there is between vision and all things that we do daily; and many times you do not realize that, by treating a problem from vision, we can solve the visual problem and the trouble that you did not know how “solve”.
What can you do if you have a visual problem?
If you have any of these problems or any other that you think that can be related to vision (if you have some question, you can consult me about it in the comments, in order to confirm if your problem is or not a visual problem that any of my colleagues may diagnose; I am sure that many people have your problem too, and if I advise you, we can help more people; but how I wrote in the welcome post, I will never give you a solution or treatment for your problem, because I would need to assess each case in an isolated way), I recommend you to visit a qualify optometrist and you ask him a comprehensive visual exam. Afterwards, he will give you the better treatment option (refractive prescription, vision therapy, reflexes therapy or rhythmic movement therapy, syntonic phototherapy... – treatments that as well I will explain at length in later posts-), or will refer you to the professional best fitted to treat your problem.
A small problem is always easier to treat than a big problem.
This idiom is very famous, but we do not always heed this advice.
Prevention and Early Detection
Optometry basically detects visual upsets, that is, visual problems, performance problems related to vision, development problems related to vision, and so on. Therefore, if this detection is made as soon as possible, the treatment will be more effective, will need to carry out it less time and the results will be more lasting.
How can you know if you suffer any visual upset?
FROM THE FACT THAT THERE IS NO OCULAR PATHOLOGY OR ILLNESS, if you notice that you have some troubles in order to see at distance or at near (in order to read, write, draw, watch TV, drive, practice any sport, use a computer,…), this indicates that probably, you are suffering from some “refractive error” (myopia, hypermetropia, astigmatism, anisometropia, presbyopia... concepts that I will explain in later posts). These visual problems are not pathologies or eye illness, but they may cause a big discomfort performing the tasks of daily life, although they have an insignificant value.
These problems are “quantitative visual disorders”, and using a prescription (eyeglasses, contact lenses or prisms), usually they are corrected (THOUGH NOT REMOVED).
But, in the other hand, there are other “problems of quality vision” (they are not eye illness neither), that we can not be shown to the patient with understandable quantitative data, but that, however, may almost cause more frustration and powerlessness than the previous problems. This is because many people do not know very well what happened, or where they can go with their problem.
Fortunately, there are more and more optician’s shops or offices where they perform visual exams are more complete than a simple ocular refraction in order to obtain those “refractive errors”. There they detect the reason of it: a performance problem at work or at school, a learning disability, a visual development problem, a clumsiness or balance problem, an inability in order to read a book during long time, a carsick, a dyslexia, and so on. I guess that you did not imagine the great relation that there is between vision and all things that we do daily; and many times you do not realize that, by treating a problem from vision, we can solve the visual problem and the trouble that you did not know how “solve”.
What can you do if you have a visual problem?
If you have any of these problems or any other that you think that can be related to vision (if you have some question, you can consult me about it in the comments, in order to confirm if your problem is or not a visual problem that any of my colleagues may diagnose; I am sure that many people have your problem too, and if I advise you, we can help more people; but how I wrote in the welcome post, I will never give you a solution or treatment for your problem, because I would need to assess each case in an isolated way), I recommend you to visit a qualify optometrist and you ask him a comprehensive visual exam. Afterwards, he will give you the better treatment option (refractive prescription, vision therapy, reflexes therapy or rhythmic movement therapy, syntonic phototherapy... – treatments that as well I will explain at length in later posts-), or will refer you to the professional best fitted to treat your problem.
A small problem is always easier to treat than a big problem.
Monday, September 22, 2008
Identifying signs and symptoms for a visual problem
Enlace a entrada en español

- General difficulties at Reading:
- General difficulties at writing or in the hand’s motor skill:
These manifestations will help you yourself to detect if any child, in your environment, may have an undiagnosed visual problem.
Moreover, in the optometric office, the professional will give you or ask you a brief questionnaire about the child, his development and his visual habits. Sometimes it is very long and tedious or even sometimes, you do not know what relation, some questions may have with the eyes or with the problem that you bring to the office; but there is not random question in these questionnaires, all of them give very important information that will help the optometrist to achieve a better diagnosis about the problem that the child has got. Therefore, even though everybody thinks that their children are wonderful and perfect, think that if you go to the office is because you suspect something, and if so, being as sincere as possible when you fill in these questionnaires is better, because the lies and half truths or half informations or underestimating the details that show where the child is not so handy, will not help; this information is the most valuable in the questionnaire.
RELATED POST
An apple a day really does keep the doctor away

Detection of visual upsets, mainly in childhood stage, is done when we observe and assess the child’s attitude and behavior when he performs a task.
- Itching, stinging or watery eyes
- Itching, stinging or watery eyes
- Blinks or rubs his eyes a lot
- Frowns or scowls in order to seeing better
- Blurred vision at distance or at near
- Frowns or scowls in order to seeing better
- Blurred vision at distance or at near
- Rigid body or moves his head forward or backward when reading or looking at a remote object
- Very close distance when watching TV, writing or reading a book
- Has difficulty for copying from the board
- Unusual eyestrain when finishing a task or decline in the reading after long periods
- Omission of tasks at near
- Fatigues quickly during reading, writing or drawing
- Bothered by the sun and lights changes
- Headache and eye pain
- Negative behavior at school or at work
- Bad head or body posture
- One eye drifts or aims at a different direction than the other (look carefully, this can be subtle). This is significant even if it only occurs when the child is tired or stressed
- Closes or covers an eye, or twists or tilts head, when reading and writing or watching TV…
- Double vision
- Very close distance when watching TV, writing or reading a book
- Has difficulty for copying from the board
- Unusual eyestrain when finishing a task or decline in the reading after long periods
- Omission of tasks at near
- Fatigues quickly during reading, writing or drawing
- Bothered by the sun and lights changes
- Headache and eye pain
- Negative behavior at school or at work
- Bad head or body posture
- One eye drifts or aims at a different direction than the other (look carefully, this can be subtle). This is significant even if it only occurs when the child is tired or stressed
- Closes or covers an eye, or twists or tilts head, when reading and writing or watching TV…
- Double vision
- General difficulties at Reading:
- Moves head when reading instead of to move the eyes
- Words slide together
- Reading speed below chronological age
- Does not understand what he has read or does not remember it
- Loses place, skips lines or rereads words or lines
- Needs to use finger as a marker to keep place
- Reads in loud voice or moving lips
- Omits or adds words or tries to guess them from the fast recognition of one part of them
- Mixes syllables when reading and numbers in maths
- Reverse letters, syllables or words
- Avoids reading or other close-up tasks
- General difficulties at writing or in the hand’s motor skill:
- Irregular and changeable letter size
- Small spacing
- Inability to write in a straight line
- Reverses letters, words and numbers when writing or copying
- Favors the reading with regard to playing or motor activities
- Favors oral exams with regards to the written ones
- When coloring, he can not keep his work inside the lines
- Does not like to draw
- Grabs the pencil badly, or takes out his tongue or does strange gestures with his face when he uses his hand to perform something that requires eye-hand coordination
- He is slow when he has to follow a dictation
- Difficulty to comprehend and perform instructions
- Bumps into things
- Sometimes he appears clumsy
- Becomes easily distracted
- Has a short attention span and needs a lot of rests
- Poor concentration
- Homework takes longer than it should
- Poor visual memory
- Negative and/ or aggressive character
- Troubles for adapting to the changes
- Gives up easily (says “I can’t”, before trying)
- Dizziness, nausea or motion sickness
- Poor posture when sitting down and working
- Incapacity of being kept sat down on a chair more of 5 minutes
- Walks on tiptoe
- Balance troubles
- Confuses right and left in himself and/or in the space past age 7 (and sometimes up and down)
- Poor performance of sports or coordination of hand-eye and foot-eye (ball skills and team games): catching and hitting a ball
- Etc.
- Bumps into things
- Sometimes he appears clumsy
- Becomes easily distracted
- Has a short attention span and needs a lot of rests
- Poor concentration
- Homework takes longer than it should
- Poor visual memory
- Negative and/ or aggressive character
- Troubles for adapting to the changes
- Gives up easily (says “I can’t”, before trying)
- Dizziness, nausea or motion sickness
- Poor posture when sitting down and working
- Incapacity of being kept sat down on a chair more of 5 minutes
- Walks on tiptoe
- Balance troubles
- Confuses right and left in himself and/or in the space past age 7 (and sometimes up and down)
- Poor performance of sports or coordination of hand-eye and foot-eye (ball skills and team games): catching and hitting a ball
- Etc.
These manifestations will help you yourself to detect if any child, in your environment, may have an undiagnosed visual problem.
Moreover, in the optometric office, the professional will give you or ask you a brief questionnaire about the child, his development and his visual habits. Sometimes it is very long and tedious or even sometimes, you do not know what relation, some questions may have with the eyes or with the problem that you bring to the office; but there is not random question in these questionnaires, all of them give very important information that will help the optometrist to achieve a better diagnosis about the problem that the child has got. Therefore, even though everybody thinks that their children are wonderful and perfect, think that if you go to the office is because you suspect something, and if so, being as sincere as possible when you fill in these questionnaires is better, because the lies and half truths or half informations or underestimating the details that show where the child is not so handy, will not help; this information is the most valuable in the questionnaire.
RELATED POST
An apple a day really does keep the doctor away
Thursday, September 04, 2008
Back to School!!!
Enlace a entrada en español

When September arrives everybody begins our “school year” –not only children-, whether we went on vacation in June, July or August, or even if we did not leave. In summer, all of us reduce our rhythm of work; the good weather, the heat, children without school, emptier and more peaceful cities, allow us to enjoy our time much more and to calm down from the frenetic rhythm of the rest of the year.
Therefore, our visual system is much more relaxed, since if our work stress decreases, as well as our visual stress decreases. On vacation, if we read is because we want to do it, or if we perform some task at near is because we are getting back to some forgotten hobby. In any of these cases, the strain is minimum and we rest when we want. So, this is the best month to check our vision. This vision will be in its purer and more relaxed state, it will give more real values both in quantity and quality of vision (refraction, focusing, fusion, perception, visual acuity, integration into other systems,…); moreover, in an emotional way, everybody is more relaxed when we are back from vacation, and everything affects.
Consequently, before going back to the intensive rhythm of all year, it is recommended to receive a complete visual exam to check that everything is right or in order to give solutions if there exists any problem before the symptoms arise, or simply in order to receive a guide from the optometrist about some good Rules of Visual Hygiene and/or of Relaxation; these are not bad things to do (I will give this rules in another post later).
The particular case of the child

But if checking that the visual system is in full performance (with nothing that disturbs it) is important in adults, imagine how important this is in the case of a child, where any visual problem can make it difficult for his right learning when reading or writing, in his hand-eye coordination, in his motor development or in his balance when he practices any sport, in his perception, in his integration of the visual information with that of other senses,… All of this will create social limitations that will be detrimental to his development, his personality and his character.
The child is in constant development and any obstacle appeared during it (in this case I write about visual development, but he would be affected by any upset of any sense that provides information that he has got to integrate), may disturb all visual information processing. It may disturb:
- the way information is received,
- the way information is integrated,
- the way information is processed,
- or even, the way received information is answered,
doing any of these actions FROM A WAY DIFFERENT THAN THE REST OF CLASSROOM CHILDREN; so, any school or daily activity (even playing with his friends) may require from himself the following: more effort, more time, more energy that makes him feel more tired, more concentration that actually makes him easily lose it when he is tired of maintaining it, more support from other senses or other skills that makes him carry certain activities in an out of balance way, and so on.
Between 0 and 14 years old detecting and treating any visual upset is very important, since constant anatomical and physiological changes are happening in the visual system as the child grows up, making the visual patterns and all neurological connections that will affect his future Perception. Also, in the first years of life, the child is learning from everything that is surrounding him, from everything that he does, and as I wrote in another post, much of this information gets in through the eyes. One visual problem (WITHOUT BEING A PATHOLOGICAL PROBLEM) may cause:
- academic performance problems,
- sport performance problems,
- school failure (to long-term),
- and the worst, self-esteem problems.
Once the visual problem has disappeared (it has been treated), these schoolchildren will improve their grades, will be happier and will be more social. They will feel with capacity to face difficult challenges in their school stage.
This is the reason why an EARLY DETECTION is so important in these ages; and both parents and teachers are responsible for detecting any small problem that the child has when he makes his daily tasks. The child will never complain because he does not know what a vision problem is, and he thinks that everybody sees like him, and if his schoolmates obtain better grades than him or play football better than him, he will simply go make a negative opinion of himself (“I am more stupid or more clumsy than the rest”), reaffirmed by the environment many times, without knowing that there is “something” that hampers him from being in the same conditions that the rest of his schoolmates or friends when he performs any activity.
One out of three children in school age suffers some kind of visual problem WITHOUT DIAGNOSING, and around 25-30% of school failure is related to visual upsets.
In the next post I will give you a list of signs and symptoms that we may take into account to detect whether your child or your pupils have some visual problem (some of that symptoms will as well valid to for the adults), but a summary, any visual problem may cause the following problems to a child:
- he can not attentively follow the teacher’s explanations in the blackboard if he does not see very well at distance,
- he can not read and study comfortably if he does not see well enough at near,
- he can not understand what he reads if he has to strain in order to read correctly,
- he will reject to go to school on a constant basis,
- his behavior will be absentminded and it will take him a lot of hard work to focus on any activity that requires a big attention,
- he will not like doing his homework,
- he will gradually feel isolated and retarded from the rest of his schoolmates with regard to his learning,
- therefore, he may make himself introverted or even develop an inferiority complex, very negative for his development as a student and as a person.
Many times parents and teachers blame these negative attitudes to psychosocial problems, to reading and writing problems (dyslexia) or to hyperactivity, when the most probable cause is just because of visual problems that have not been treated.
Although a child had not developed his visual system in a normal way, the sooner we detect the problem, the sooner we will be able to treat it and to help him promote his visual system, getting back to his normal development level for the child’s age. This happens because the younger the child is, the more plastic his visual system is, due to that although the visual organ develops completely at 2 years old, until 5 years old his visual system is not completely functional. So, if during this period his vision suffers any upset (myopia, astigmatism, eye deviation, lazy eye, retained primitive reflex,…), the development will not be the same, and if it is not treated on time, it will cause difficulties in his daily life. We can not allow for the time to go by and see if the problem is solved by itself, BECAUSE THIS WILL NOT HAPPEN, it will increase and it may be too late when we want to do anything.
Also, it may happen that, currently, the child has not had any problem at school and we think that his vision is perfect, and his parents decide that he does not need any visual check WHILE HE DOES NOT SHOW ANY PROBLEM AT SCHOOL. We must not wait for this moment to happen: a routine check is not bad for anybody and it can avoid that the symptoms and the performance problems at school rise. It may happen that in previous academic years the child had no problems, but as the new year passes by, he shows performance problems or bad grades that he did not have until that moment. That may simply mean that the child has a latent visual problem that was not obvious until that moment because the academic demand was not sufficiently high to show it. But when the academic demand increases, the level increases, and a visual problem that seems in control is suddenly out of hand. For instance, because the effort for understanding a more complicated text may show a reading problem that it seemed it did not exist before.
Owing to all these previous facts, as an optometrist I recommend that all of us should receive a visual check at least once a year, CHILDREN SPECIALLY. And when I write “visual check” I do not simply mean going to an ophthalmologist – which is also recommended, in order to be sure that our eyes are in a healthy state-, but to a qualified optometrist capable to assess if his visual system is ready for working in full performance.
Any visual upset in children or adults, causes our vision not to be efficient and, consequently our learning or work will neither be.

When September arrives everybody begins our “school year” –not only children-, whether we went on vacation in June, July or August, or even if we did not leave. In summer, all of us reduce our rhythm of work; the good weather, the heat, children without school, emptier and more peaceful cities, allow us to enjoy our time much more and to calm down from the frenetic rhythm of the rest of the year.
Therefore, our visual system is much more relaxed, since if our work stress decreases, as well as our visual stress decreases. On vacation, if we read is because we want to do it, or if we perform some task at near is because we are getting back to some forgotten hobby. In any of these cases, the strain is minimum and we rest when we want. So, this is the best month to check our vision. This vision will be in its purer and more relaxed state, it will give more real values both in quantity and quality of vision (refraction, focusing, fusion, perception, visual acuity, integration into other systems,…); moreover, in an emotional way, everybody is more relaxed when we are back from vacation, and everything affects.
Consequently, before going back to the intensive rhythm of all year, it is recommended to receive a complete visual exam to check that everything is right or in order to give solutions if there exists any problem before the symptoms arise, or simply in order to receive a guide from the optometrist about some good Rules of Visual Hygiene and/or of Relaxation; these are not bad things to do (I will give this rules in another post later).
The particular case of the child

But if checking that the visual system is in full performance (with nothing that disturbs it) is important in adults, imagine how important this is in the case of a child, where any visual problem can make it difficult for his right learning when reading or writing, in his hand-eye coordination, in his motor development or in his balance when he practices any sport, in his perception, in his integration of the visual information with that of other senses,… All of this will create social limitations that will be detrimental to his development, his personality and his character.
The child is in constant development and any obstacle appeared during it (in this case I write about visual development, but he would be affected by any upset of any sense that provides information that he has got to integrate), may disturb all visual information processing. It may disturb:
- the way information is received,
- the way information is integrated,
- the way information is processed,
- or even, the way received information is answered,
doing any of these actions FROM A WAY DIFFERENT THAN THE REST OF CLASSROOM CHILDREN; so, any school or daily activity (even playing with his friends) may require from himself the following: more effort, more time, more energy that makes him feel more tired, more concentration that actually makes him easily lose it when he is tired of maintaining it, more support from other senses or other skills that makes him carry certain activities in an out of balance way, and so on.
Between 0 and 14 years old detecting and treating any visual upset is very important, since constant anatomical and physiological changes are happening in the visual system as the child grows up, making the visual patterns and all neurological connections that will affect his future Perception. Also, in the first years of life, the child is learning from everything that is surrounding him, from everything that he does, and as I wrote in another post, much of this information gets in through the eyes. One visual problem (WITHOUT BEING A PATHOLOGICAL PROBLEM) may cause:
- academic performance problems,
- sport performance problems,
- school failure (to long-term),
- and the worst, self-esteem problems.
Once the visual problem has disappeared (it has been treated), these schoolchildren will improve their grades, will be happier and will be more social. They will feel with capacity to face difficult challenges in their school stage.
This is the reason why an EARLY DETECTION is so important in these ages; and both parents and teachers are responsible for detecting any small problem that the child has when he makes his daily tasks. The child will never complain because he does not know what a vision problem is, and he thinks that everybody sees like him, and if his schoolmates obtain better grades than him or play football better than him, he will simply go make a negative opinion of himself (“I am more stupid or more clumsy than the rest”), reaffirmed by the environment many times, without knowing that there is “something” that hampers him from being in the same conditions that the rest of his schoolmates or friends when he performs any activity.
One out of three children in school age suffers some kind of visual problem WITHOUT DIAGNOSING, and around 25-30% of school failure is related to visual upsets.
In the next post I will give you a list of signs and symptoms that we may take into account to detect whether your child or your pupils have some visual problem (some of that symptoms will as well valid to for the adults), but a summary, any visual problem may cause the following problems to a child:
- he can not attentively follow the teacher’s explanations in the blackboard if he does not see very well at distance,
- he can not read and study comfortably if he does not see well enough at near,
- he can not understand what he reads if he has to strain in order to read correctly,
- he will reject to go to school on a constant basis,
- his behavior will be absentminded and it will take him a lot of hard work to focus on any activity that requires a big attention,
- he will not like doing his homework,
- he will gradually feel isolated and retarded from the rest of his schoolmates with regard to his learning,
- therefore, he may make himself introverted or even develop an inferiority complex, very negative for his development as a student and as a person.
Many times parents and teachers blame these negative attitudes to psychosocial problems, to reading and writing problems (dyslexia) or to hyperactivity, when the most probable cause is just because of visual problems that have not been treated.
Although a child had not developed his visual system in a normal way, the sooner we detect the problem, the sooner we will be able to treat it and to help him promote his visual system, getting back to his normal development level for the child’s age. This happens because the younger the child is, the more plastic his visual system is, due to that although the visual organ develops completely at 2 years old, until 5 years old his visual system is not completely functional. So, if during this period his vision suffers any upset (myopia, astigmatism, eye deviation, lazy eye, retained primitive reflex,…), the development will not be the same, and if it is not treated on time, it will cause difficulties in his daily life. We can not allow for the time to go by and see if the problem is solved by itself, BECAUSE THIS WILL NOT HAPPEN, it will increase and it may be too late when we want to do anything.
Also, it may happen that, currently, the child has not had any problem at school and we think that his vision is perfect, and his parents decide that he does not need any visual check WHILE HE DOES NOT SHOW ANY PROBLEM AT SCHOOL. We must not wait for this moment to happen: a routine check is not bad for anybody and it can avoid that the symptoms and the performance problems at school rise. It may happen that in previous academic years the child had no problems, but as the new year passes by, he shows performance problems or bad grades that he did not have until that moment. That may simply mean that the child has a latent visual problem that was not obvious until that moment because the academic demand was not sufficiently high to show it. But when the academic demand increases, the level increases, and a visual problem that seems in control is suddenly out of hand. For instance, because the effort for understanding a more complicated text may show a reading problem that it seemed it did not exist before.
Owing to all these previous facts, as an optometrist I recommend that all of us should receive a visual check at least once a year, CHILDREN SPECIALLY. And when I write “visual check” I do not simply mean going to an ophthalmologist – which is also recommended, in order to be sure that our eyes are in a healthy state-, but to a qualified optometrist capable to assess if his visual system is ready for working in full performance.
Any visual upset in children or adults, causes our vision not to be efficient and, consequently our learning or work will neither be.
Tuesday, August 26, 2008
And again in Spain…
I resume the posts after not being able to write in this blog during more than one month. The reasons have been, in one hand, that I’ve moved to my country again (our American adventure, after one year and a half, has finally finished :-( ); and in the other hand, that some serious family problems are taking all of my time. Because of this last reason, I hope I can recover the publishing rhythm, but if my articles take a long time to be posted, do not think that I have forgotten the blog. I enjoy writing it, and if nothing stops me, I will write as soon as I can.
Monday, July 21, 2008
What other types of information get in through our eyes?
Enlace a entrada en español.
Besides the four important routes that the visual information makes to process it (and that I already showed you in the previous post), there are certain stimuli that get in through the eyes and also that go to other nervous system pathways to cause the right answers.
EXAMPLE 1:
When we get across a tunnel, we turn on the car headlights on, but even so, our eyes have to get used to the sudden decrease of the light in order to see clearly again, and drive safely.
In order to achieve this action, this information arrives to the PRETECTUM (a structure in the mesencephalon next to the Superior Colliculus). This structure sends the information about “poor light”, to the EDINGER-WESTPHAL NUCLEUS and from there, finally to the CILIARY GANGLION. This last structure sends a command to the DILATOR MUSCLE of the iris, in order to increase the pupil size (i.e. it dilates), and so, to get more light into the eye. Thus, the rods of the retina are stimulated, and they give us the information that we need in order to keep on driving in those conditions.
Besides the four important routes that the visual information makes to process it (and that I already showed you in the previous post), there are certain stimuli that get in through the eyes and also that go to other nervous system pathways to cause the right answers.
EXAMPLE 1:
When we get across a tunnel, we turn on the car headlights on, but even so, our eyes have to get used to the sudden decrease of the light in order to see clearly again, and drive safely.
In order to achieve this action, this information arrives to the PRETECTUM (a structure in the mesencephalon next to the Superior Colliculus). This structure sends the information about “poor light”, to the EDINGER-WESTPHAL NUCLEUS and from there, finally to the CILIARY GANGLION. This last structure sends a command to the DILATOR MUSCLE of the iris, in order to increase the pupil size (i.e. it dilates), and so, to get more light into the eye. Thus, the rods of the retina are stimulated, and they give us the information that we need in order to keep on driving in those conditions.

When we get out the tunnel, the process is shorter. The information about “much light”, stops in the EDINGER-WESTPHAL NUCLEUS, who sends a command to the SPHINTER MUSCLE of the iris in order for the pupil to decrease its size (i.e. it contracts), less light gets into the eyes and therefore so we are not dazzled at all so we can see clearly quickly.
EJEMPLO 2:
The “STOP” sign one: Everything gets inside through the eyes, but as I explained in the previous post, the Lateral Geniculate Nucleus (LGN), is responsible for filtering this information so that the brain is not saturated with unnecessary information. So, the ATTENTION is involved in this process and that “attentional window” is controlled through another nucleus placed in the Thalamus: PULVINAR.
There are two routes: in one hand, the route that “facilitates the attention” and that leads it to one or another object (the STOP sign, the white line, the car in front of us…) or increase its attention range (we pay attention to everything surrounding us, to what is the car that has priority to get out of the STOP sign cross in the first place,….). And this information passes through the Pulvinar.
In the other hand, the route that “inhibits the attention” (children playing in the car behind, the shopping bag that falls over when we press the brake,…). This route is direct between the Lateral Geniculate Nucleus and the Occipital Lobe.
These routes are MAGNO, that is, unconscious routes. Fortunately we do not have to control consciously everything at the same time and many of previous routes: if we had to, a simple “STOP” sign will be chaotic.
But besides these examples or these nervous structures, there are many others with the same importance, that are also involved in this visual information processing.
For instance, the CEREBELLUM. It is the structure responsible for the coordination, the balance and the movement; therefore, it allows us to do precise movements in order to position the car right before the white line, put our hand on the wheel, put our foot on the brake pedal,…
Another example is the HIPPOCAMPUS. It is a structure located in the medial temporal lobe and is structure responsible for long and short term memory; therefore, it allows us to remember what the traffic sign means, what we have to do before it, what streets we have to take to arrive to our office, what breakfast we had breakfast this morning,…
As you see, when we are driving a car it is not only important the “what” but also the “where”, that is, we not only see the sign and see it clear, but also to need to know and interpret it: recognizing it, identifying it, remembering it, relating to the rest of information that we have, ignoring whatever it does not contribute, knowing how to act before it, knowing what we can or must do, how long and where we can move according to where we are,…
That is, in order to drive a car, to play tennis or just to walk or to move from one place to another, if we only have a picture of the things that we see, our brain can not make those judgements that are so necessary.
RELATED POST
Where does what we see go? - Visual Information Processing (from the eye to the brain)
Monday, July 14, 2008
Where does what we see go? - Visual Information Processing (from the eye to the brain)
Enlace a entrada en español.
I am sure much of you think the image stops in the eye, that is, that this is where the process ends. We see with the eyes, don’t we? But maybe, after you read the previous post, your thoughts are confused.
In the other hand, I am sure some of you know that the brain is involved in this process but you do not know or understand very well how the connection is between eyes and brain.
It is true that this process is complicated ENOUGH, that is why, so it is easier to understand, I will show how what we see is processed from a practical example and with some graphics.
I am sure much of you think the image stops in the eye, that is, that this is where the process ends. We see with the eyes, don’t we? But maybe, after you read the previous post, your thoughts are confused.
In the other hand, I am sure some of you know that the brain is involved in this process but you do not know or understand very well how the connection is between eyes and brain.
It is true that this process is complicated ENOUGH, that is why, so it is easier to understand, I will show how what we see is processed from a practical example and with some graphics.
 Let’s suppose we are driving on a street and we are arriving to a cross. In the corner we see the “STOP” traffic sign.
Let’s suppose we are driving on a street and we are arriving to a cross. In the corner we see the “STOP” traffic sign.
I am going to show you how much information is processed just when seeing this simple traffic sign.
- In the first instance, we have the VISUAL PROCESS itself, that is, obtaining the clear image.
If you remember the previous post, the image created in both eye foveas is processed by the cones (A) that are in the central area of the retina. They send the information to the parvo ganglion cells (C) and leave the eye across the optic nerve (11) . These ganglion cells take the information about the color, bright, clarity and contrast of the STOP traffic sign to the LATERAL GENICULATE NUCLEUS. This is a relief and control station in the visual pathway: almost all information -that the parvo ganglion cells receive-arrives here, and this structure filters and leads it towards the respective places in the brain. So, only ten percent of this visual information is sent to the OCCIPITAL LOBE or VISUAL CORTEX, in order to create the image.
This particular process is incredibly much more complex, but by now, this is enough to understand the rest of the visual information processing
______________________________________
The rest of the pathways that take part in this visual information processing, are not called “visual pathways”, because the information does not go to the occipital lobe directly. The following information that is processed, is not purely visual, although the information had been obtained through the eyes.
- Therefore, in the second instance, we have the following PROCESS: EYES -> SUPERIOR COLLICULUS -> PARIETAL LOBE. In this process the information about “Where am I?” is obtained:
This pathway is made up basically of magno ganglion cells (C) that received the information from the rods in both retinas.
The Superior Colliculus is a paired structure of the nervous system placed in the mesencephalon (2) , right under the thalamus. The Superior Colliculus belongs to the Brainstem, which is the structure that joins the Brain and the Spinal Cord.
It deals to integrate the visual input with the auditory, somaticsensory (about balance and proprioception, among others) and tactile input; and thus we achieve the information about “Where are we?”.
In order to answer this question, the Superior Colliculus makes eyes and head move automatically towards the stimuli in the environment.
In the practical example, the group of all information is processed so that the Posterior Parietal Lobe allows us to calculate our movement, the speed of our car, the strength that we need to do in order to put our foot on the brake pedal, the direction of our car, or the rest of the cars, where our feet are, where our hands are, where we have to stop near the traffic sign… This lobe give us a metal spatial map about ourselves.
Therefore, when we have a car crash with a collision from behind, our head suffers a “lash” front to back, and in this case, the part of the brain is usually is affected is the mesencephalon, so, as well as we suffer strong cervical pains after the accident, it is also frequent to suffer disorientation, poor concentration, panicky feeling in places with crowd or difficulty for going up or down stairs. These are symptoms that seems light and that many people might not attribute to the car crash, but they make their daily life difficult. We can help these people by using Vision Therapy to get back the lost stability back.
- In the third instance, we have the following PROCESS: OCCIPITAL LOBE -> -> POSTERIOR PARIETAL LOBE. In this process the information about “Where is the object?” -the traffic sign-, is obtained:
The information from magno ganglion cells that arrives to the occipital lobe, does not stop here; some of these mango ganglion cells (C) go to Medial Temporal Lobe and, from there, go to the posterior parietal lobe to give us some information about “Where is the stop?”: Where is the line? Where must we stop? Where is the brake pedal to put our foot? Where is the car behind us or in front us?... As I explained above, Parietal Lobe allows us to make special calculations, as in the previous process. This lobe gives us a mental spatial map about our environment.
The information about “Where am I?” and “Where is the object?” allows the parietal lobe to make a motor plan, that is, “how we must do the things”. This lobe allows us to look at the road in the mean time: we look at the mirrors, we turn the wheel if it is necessary, we keep on the security distance regarding the front car, turn on the headlights if we get into a tunnel, we talk to another person in the car, we listen to the radio,...
But if you think about it, this process is carried out unconsciously, that is, all information that comes from the peripheral retina (Magno system) is processed and is carried out automatically. The same thing happens when we are driving on a road and we find an obstacle in our lane; then we look at the rear mirror and if there is not any further risk, we slightly turn the wheel to avoid it.
The responsible lobe for carrying out this action is the parietal one, but we have to do that unconsciously, as a reflex.
When we want to pass another car in the road and we have another one in the opposite direction, this lobe gives us some information about the following: what speed is the other car going at? What speed is the front car going at? What speed is our car going at? What car is moving faster? Do we have enough time to pass without risk?...
- Finally, in the fourth instance, we have the following PROCESS: OCCIPITAL LOBE -> INFERIOR TEMPORAL LOBE. In this process, the information about “What is the object?” -the traffic sign-, is obtained:
Some of the information that arrives to occipital lobe through the parvo ganglion cells (C) from both retinas, do not stop here, they goes to the inferior temporal lobe in order to give us information about what we are seeing: the ”STOP” traffic sign. This information helps us identify what we see: it is a traffic sign, what kind of traffic sign is or what it means; and thus we can know how we have to answer (according to our experience).
This lobe is responsible for the language, that is why, it helps us to give a meaning to the things.
________________________________________
These are the four basic routes, but many others are created in the brain at the same time. I will show some of them in the next post, that it will be posted sooner than usual.
As you see, the brain is so complex and I have just showed you one part. But among many strange names of nervous structures (that I repeat, you do not need to remember), what I want you is to realize that in a few seconds, our brain works 100% and that there are maaaaany activities generated inside; this way, it is able to very effective receive, process and answer from what we see if the visual information processing is correct.
RELATED POST
What other types of information get in through our eyes?
Wednesday, June 25, 2008
A little bit of basic ocular anatomy… The Retina.
Enlace a entrada en español
As I wrote in the first post of this series about “Basic Ocular Anatomy”, the retina (10) is a layer of the eye that deserves one blog post just to itself.
It is the most important layer of the eye, because it contributes to the first part of the Visual Information Processing that we receive: the formation of the image, which will be processed later on.
I am going to show the retina from different points of view, in order for it to be easier to understand. Its importance is appropriate to its complexity.

In one hand, in order to understand how the eye works, you must think about it as an “old picture camera” (that is, with film ;-)); just as the image is expressed in the camera film, it is expressed in the eye retina.
 In the other hand, you must also think that the eye behaves as a “dark chamber”; this consists for example, of a dark box which has a little hole in one of its walls (as the pupil in the eye). In opposite wall (as the retina in the eye) an inverted image is made from the external objects.
In the other hand, you must also think that the eye behaves as a “dark chamber”; this consists for example, of a dark box which has a little hole in one of its walls (as the pupil in the eye). In opposite wall (as the retina in the eye) an inverted image is made from the external objects.
One eye without any problem of refraction (myopia, hyperopia or astigmatism), that looks at distance (more than fifteen feet), is at a state of rest. The iris (2) behaves as a camera diaphragm, whose contraction controls the quantity of light that gets into it through the pupil (3); in this situation, the lens (8), the other dynamic part of the eye, is at rest. Therefore, the human eye does not have to strain when it looks at distance.
When one person looks at near, if these dynamic parts of the eye do not modify their state, he will see blurred. It is the same thing that happens if the lens of a camera does not modify its focusing in order to clear a close object (after focusing something that was far): the picture will be blurred.
In the eye, in order to clear a close object, the thickness of the crystalline lens (8) varies. This mechanism is called accommodation, but I will write about this later.
When we look distant something as well as close something, this has to get to the film inside of a camera, or to the retina in the eye, in order to achieve a clear image.
Once you have understood how the eye works, now I am going to show you how the light gets into it, and it reaches the retina (10):
 The light thrown by one object converges on the cornea (1), passes through the pupil (3), and gets to the crystalline lens (8). At this point, the image is inverted (according to the optics laws). If there is no reaction in the lens, the image that reaches the retina(10) can be more or less blurred, depending on the distance to the object (considering that this is not further than fifteen feet, as I explained before). That way if the image is blurred, this information gets to the brain and it answers by sending a command to the crystalline lens in order to modify its shape and therefore, allowing the image to get to the retina, thus creating a clear image. This action happens automatically and the process is very fast; it is similar to the autofocus process of a picture camera, which focuses automatically on what it detects in the central framing of the viewfinder.
The light thrown by one object converges on the cornea (1), passes through the pupil (3), and gets to the crystalline lens (8). At this point, the image is inverted (according to the optics laws). If there is no reaction in the lens, the image that reaches the retina(10) can be more or less blurred, depending on the distance to the object (considering that this is not further than fifteen feet, as I explained before). That way if the image is blurred, this information gets to the brain and it answers by sending a command to the crystalline lens in order to modify its shape and therefore, allowing the image to get to the retina, thus creating a clear image. This action happens automatically and the process is very fast; it is similar to the autofocus process of a picture camera, which focuses automatically on what it detects in the central framing of the viewfinder.
So, after the light passes through the gelatinous vitreous humor (9), it will reach the end of the route in the eye: the retina (10); in this point the image is clear (I will explain later which are the cases where the image is not clear and why).
But unlike a picture camera, the image does not just stay in the retina. This eye’s innermost nervous layer is the one responsible for converting the photons of the light that it receives into nervous signals that can be relayed to the brain; there it interprets them and gives them a right meaning. Therefore, the brain is the part responsible for “developing the film”, that is, interpreting it (knowing what the object is, what it means to us, what emotion causes, how to answer before it, and so on).
In order to achieve this transformation, the retina (10) is composed of five kinds of nervous cells, which collect all luminous information. They are not just responsible for making the image clear, but they also extract the basic information of the object about its color, its shape, its orientation, its movement, transmitting it to the brain. The human eye transmits visual data to the brain at about the same speed as two computers can share data.
These cells are placed in the retina in different layers, but as I do not want to make it very complicated, I am just going to point out three of them:

The light passes through all retina nervous layers to reach the outermost one: the one composed by photoreceptors (called rods and cones) (A); there the incoming light is reflected and passes through the retina again in the opposite direction, transforming this light into nervous impulses and transmitting the neurological information through different layers of nervous cells to reach the last one: ganglion cells (C); in this layer their thin axons bundle together in order to get out the eye and to the Optic Nerve (11) and send the impulses to the brain, thus starting, the VISUAL PATH.
There are two subtype of photoreceptors: rods and cones (A) distributed by the whole retina, where each one has a certain function and location.
- Neither of them exists in the point of the ganglion cells exit (Blind Spot -12-).
- Cone cells are found mainly in the central area of the retina, because they are the cells responsible for the details (the clarity, the shape and the color) of the object. This central area of the retina is where the eye “machine” leads the image of an object, in order to see it clear and with 20/20 of vision. This central area is the macula (14) (http://rosavisionenglish.blogspot.com/2008/05/little-bit-of-basic-ocular-anatomy-eye.html) and its central point with higher vision in the retina is the fovea (13) (http://rosavisionenglish.blogspot.com/2008/05/little-bit-of-basic-ocular-anatomy-eye.html). As these cells are the ones responsible to catch the details, they work better with well-light conditions. So, some activities where these cells are used are for instance, when reading or writing.
- Rod cells, in the other hand, are found mainly in the peripheral area. As we get away from the macula (14), the quantity of cones decreases and the quantity of rods increases. In the peripheral area the information about the clarity or the color is not so important, but detecting the orientation or the movement of the object that we look at. Therefore, these cells are stimulated with low-light conditions. Also, these cells are very sensitive to changes in contrast even at low-light level.
These photoreceptors (A) at the same time, stimulate certain ganglion cells (C); that is, each type of photoreceptor stimulates one type of ganglion cell, so each cell takes a certain information; both information elements travel parallelly to different areas of the brain, and once there, all information is mixed. The brain gives the meaning of the world surrounding us: where the object is, what it is, how big is, what color it is, how far it is,… It takes all information from the world and puts it together, in order to find similarities and differences, compare, discriminate and so on.
Consequently, in one hand, CONES (A) send information to PARVO ganglion cells (C), which take the information about the shape, the color and the detail, that is, what the object is; they help us identify and take out a meaning; help to see that object clearly (the Visual Acuity) and they work better if the object is stopped.
In the other hand, RODS (A) send information to MAGNO ganglion cells (C), which take information about the movement, the space and the orientation; that is, they report on the movement direction, its speed, calculate distances, where the object is, where I am and three-dimensionality. They help us move ourselves inside a dark room avoiding that we hit ourselves with other objects, or avoiding that we crash with the things that we do not look at directly (for example, with the doorframe when we go through it without looking at it), and so on.
As you can see, we do not just “see” the objects, or rather, we do not just see them clear or blurred; what a retina catches from an object, that image, is not only a picture, goes along with much more information and it all begins to be processed in the retina. But the rest of this complex but amazing processing of visual information that happens in the brain, will be explained it in the next post…
RELATED POSTS
A little bit of basic ocular anatomy… Eye or Ocular Globe
A little bit of basic ocular anatomy… What is the eye surrounded by?
As I wrote in the first post of this series about “Basic Ocular Anatomy”, the retina (10) is a layer of the eye that deserves one blog post just to itself.
It is the most important layer of the eye, because it contributes to the first part of the Visual Information Processing that we receive: the formation of the image, which will be processed later on.
I am going to show the retina from different points of view, in order for it to be easier to understand. Its importance is appropriate to its complexity.

In one hand, in order to understand how the eye works, you must think about it as an “old picture camera” (that is, with film ;-)); just as the image is expressed in the camera film, it is expressed in the eye retina.
 In the other hand, you must also think that the eye behaves as a “dark chamber”; this consists for example, of a dark box which has a little hole in one of its walls (as the pupil in the eye). In opposite wall (as the retina in the eye) an inverted image is made from the external objects.
In the other hand, you must also think that the eye behaves as a “dark chamber”; this consists for example, of a dark box which has a little hole in one of its walls (as the pupil in the eye). In opposite wall (as the retina in the eye) an inverted image is made from the external objects.One eye without any problem of refraction (myopia, hyperopia or astigmatism), that looks at distance (more than fifteen feet), is at a state of rest. The iris (2) behaves as a camera diaphragm, whose contraction controls the quantity of light that gets into it through the pupil (3); in this situation, the lens (8), the other dynamic part of the eye, is at rest. Therefore, the human eye does not have to strain when it looks at distance.
When one person looks at near, if these dynamic parts of the eye do not modify their state, he will see blurred. It is the same thing that happens if the lens of a camera does not modify its focusing in order to clear a close object (after focusing something that was far): the picture will be blurred.
In the eye, in order to clear a close object, the thickness of the crystalline lens (8) varies. This mechanism is called accommodation, but I will write about this later.
When we look distant something as well as close something, this has to get to the film inside of a camera, or to the retina in the eye, in order to achieve a clear image.
Once you have understood how the eye works, now I am going to show you how the light gets into it, and it reaches the retina (10):
 The light thrown by one object converges on the cornea (1), passes through the pupil (3), and gets to the crystalline lens (8). At this point, the image is inverted (according to the optics laws). If there is no reaction in the lens, the image that reaches the retina(10) can be more or less blurred, depending on the distance to the object (considering that this is not further than fifteen feet, as I explained before). That way if the image is blurred, this information gets to the brain and it answers by sending a command to the crystalline lens in order to modify its shape and therefore, allowing the image to get to the retina, thus creating a clear image. This action happens automatically and the process is very fast; it is similar to the autofocus process of a picture camera, which focuses automatically on what it detects in the central framing of the viewfinder.
The light thrown by one object converges on the cornea (1), passes through the pupil (3), and gets to the crystalline lens (8). At this point, the image is inverted (according to the optics laws). If there is no reaction in the lens, the image that reaches the retina(10) can be more or less blurred, depending on the distance to the object (considering that this is not further than fifteen feet, as I explained before). That way if the image is blurred, this information gets to the brain and it answers by sending a command to the crystalline lens in order to modify its shape and therefore, allowing the image to get to the retina, thus creating a clear image. This action happens automatically and the process is very fast; it is similar to the autofocus process of a picture camera, which focuses automatically on what it detects in the central framing of the viewfinder.So, after the light passes through the gelatinous vitreous humor (9), it will reach the end of the route in the eye: the retina (10); in this point the image is clear (I will explain later which are the cases where the image is not clear and why).
But unlike a picture camera, the image does not just stay in the retina. This eye’s innermost nervous layer is the one responsible for converting the photons of the light that it receives into nervous signals that can be relayed to the brain; there it interprets them and gives them a right meaning. Therefore, the brain is the part responsible for “developing the film”, that is, interpreting it (knowing what the object is, what it means to us, what emotion causes, how to answer before it, and so on).
In order to achieve this transformation, the retina (10) is composed of five kinds of nervous cells, which collect all luminous information. They are not just responsible for making the image clear, but they also extract the basic information of the object about its color, its shape, its orientation, its movement, transmitting it to the brain. The human eye transmits visual data to the brain at about the same speed as two computers can share data.
These cells are placed in the retina in different layers, but as I do not want to make it very complicated, I am just going to point out three of them:

The light passes through all retina nervous layers to reach the outermost one: the one composed by photoreceptors (called rods and cones) (A); there the incoming light is reflected and passes through the retina again in the opposite direction, transforming this light into nervous impulses and transmitting the neurological information through different layers of nervous cells to reach the last one: ganglion cells (C); in this layer their thin axons bundle together in order to get out the eye and to the Optic Nerve (11) and send the impulses to the brain, thus starting, the VISUAL PATH.
There are two subtype of photoreceptors: rods and cones (A) distributed by the whole retina, where each one has a certain function and location.
- Neither of them exists in the point of the ganglion cells exit (Blind Spot -12-).
- Cone cells are found mainly in the central area of the retina, because they are the cells responsible for the details (the clarity, the shape and the color) of the object. This central area of the retina is where the eye “machine” leads the image of an object, in order to see it clear and with 20/20 of vision. This central area is the macula (14) (http://rosavisionenglish.blogspot.com/2008/05/little-bit-of-basic-ocular-anatomy-eye.html) and its central point with higher vision in the retina is the fovea (13) (http://rosavisionenglish.blogspot.com/2008/05/little-bit-of-basic-ocular-anatomy-eye.html). As these cells are the ones responsible to catch the details, they work better with well-light conditions. So, some activities where these cells are used are for instance, when reading or writing.
- Rod cells, in the other hand, are found mainly in the peripheral area. As we get away from the macula (14), the quantity of cones decreases and the quantity of rods increases. In the peripheral area the information about the clarity or the color is not so important, but detecting the orientation or the movement of the object that we look at. Therefore, these cells are stimulated with low-light conditions. Also, these cells are very sensitive to changes in contrast even at low-light level.
These photoreceptors (A) at the same time, stimulate certain ganglion cells (C); that is, each type of photoreceptor stimulates one type of ganglion cell, so each cell takes a certain information; both information elements travel parallelly to different areas of the brain, and once there, all information is mixed. The brain gives the meaning of the world surrounding us: where the object is, what it is, how big is, what color it is, how far it is,… It takes all information from the world and puts it together, in order to find similarities and differences, compare, discriminate and so on.
Consequently, in one hand, CONES (A) send information to PARVO ganglion cells (C), which take the information about the shape, the color and the detail, that is, what the object is; they help us identify and take out a meaning; help to see that object clearly (the Visual Acuity) and they work better if the object is stopped.
In the other hand, RODS (A) send information to MAGNO ganglion cells (C), which take information about the movement, the space and the orientation; that is, they report on the movement direction, its speed, calculate distances, where the object is, where I am and three-dimensionality. They help us move ourselves inside a dark room avoiding that we hit ourselves with other objects, or avoiding that we crash with the things that we do not look at directly (for example, with the doorframe when we go through it without looking at it), and so on.
As you can see, we do not just “see” the objects, or rather, we do not just see them clear or blurred; what a retina catches from an object, that image, is not only a picture, goes along with much more information and it all begins to be processed in the retina. But the rest of this complex but amazing processing of visual information that happens in the brain, will be explained it in the next post…
RELATED POSTS
A little bit of basic ocular anatomy… Eye or Ocular Globe
A little bit of basic ocular anatomy… What is the eye surrounded by?
Subscribe to:
Posts (Atom)






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
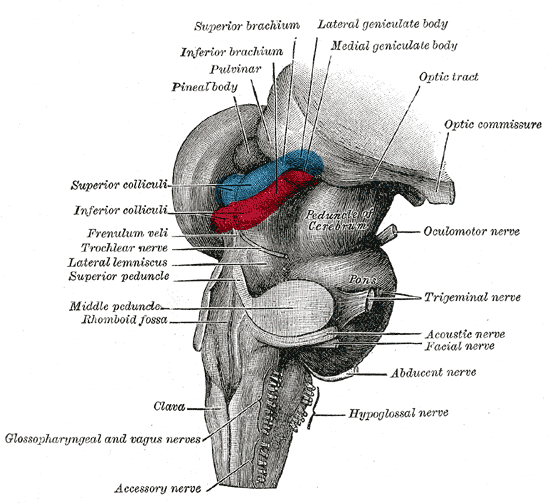{kind=link}
{kind=link}
{kind=link}